
From Resistance to Response: When the Trial Fails, But the Patient Doesn't
Exploring vagal nerve stimulation for treatment resistant depression

It reads like a slam-dunk headline: “Vagus nerve implant shows lasting benefit for treatment-resistant depression, two-year study finds.” However, despite impressive durability, the trial failed to meet its primary goal on the standard depression scale. The vagus nerve, last seen in Field Note 1 as a player in mouse memory loss, returns here in a related but very different role. And it raises a tough question about whether this is a story about the benefits of vagus nerve stimulation or more about the challenge of assessing people who have spent half their lives trying depression treatments that fail them

“The vagus nerve paradoxically appears to be a major contributor to both mental illness and wellness.”
Ever since doing research for Field Note 1 on how gut bacteria, the vagus nerve, inflammation, and short-term memory interact in mice, my Facebook feed has been overflowing with ads for vagus nerve stimulators. Beware, you, too, are now destined for the same advertising purgatory!
It’s intriguing to me that the vagus nerve paradoxically appears to be a major contributor to both mental illness and wellness, leading me to this two-year study on Vagal Nerve Stimulation (VNS) for people with Treatment-Resistant Depression (TRD).
My impression has always been that one is labeled with TRD only until they find the right treatment. But what’s the right number of treatments to try? The patients in this trial went through an average of 13.5 lifetime failed antidepressant treatments. Approximately 41% had a prior suicide attempt, and had lived roughly half their lives in depression; many had also failed Transcranial Magnetic Stimulation (TMS) or Electroconvulsive Therapy (ECT). To underscore the severity of the situation, 72% of participants were unemployed.
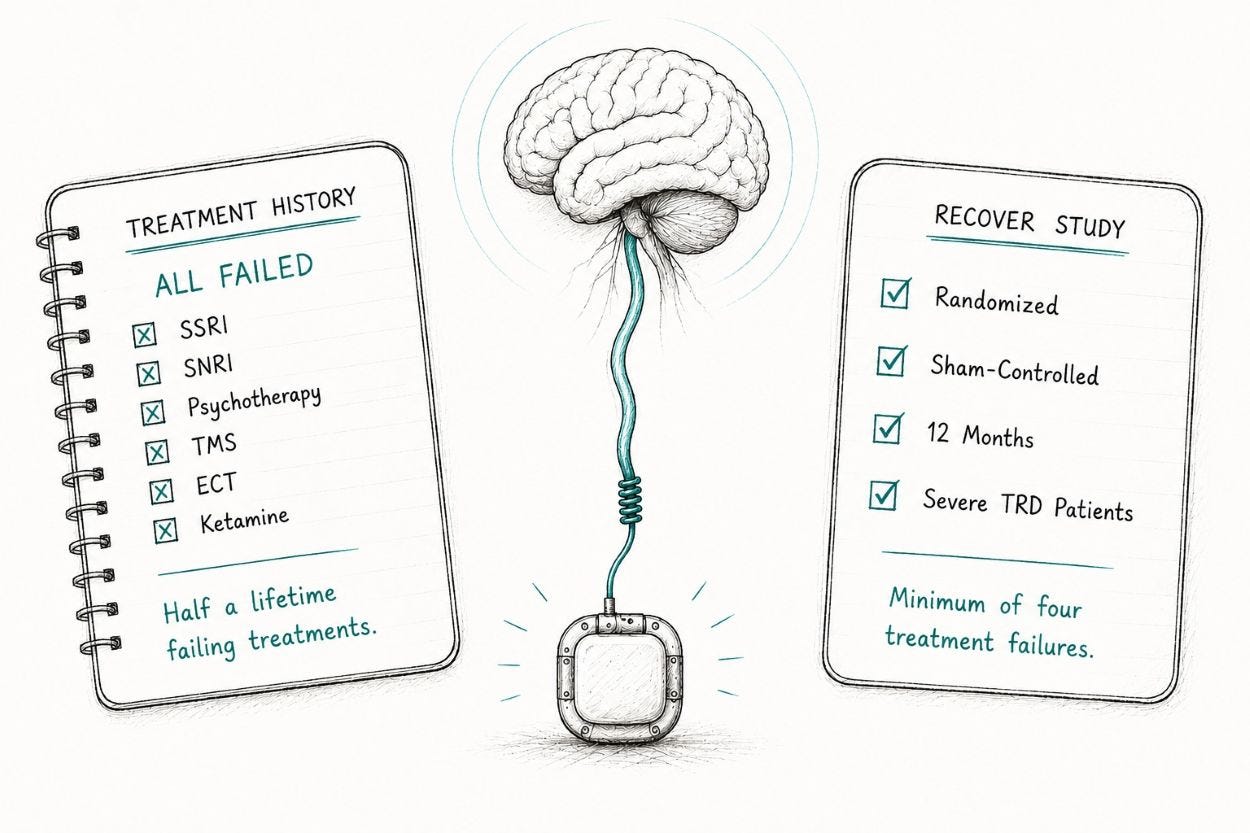
My heart goes out to these people. Study qualification requires “failing four or more antidepressants,” which I think is backward because it places the burden on the patient. The treatments failed them, fitting into my upstream hypothesis.
The way I see it, every downstream depression treatment available today is a hammer. For most people, finding the right hammer for their nail works. With TRD, your depression is more like a screw, and, with only hammers to choose from, you are screwed.
As the authors touch on, TRD may be a totally different beast than other types of depression, which raises the question of whether the standard tools for measuring depression are the right ones for this population.

VNS has a 20-year regulatory history, originally developed for drug-resistant epilepsy. Researchers later discovered its antidepressant effects, leading the FDA to approve VNS for TRD in 2005. This VNS is not something you clip to your ear or wear on your neck. It’s a surgical procedure that, despite FDA approval, is largely unavailable because, in 2007, the Centers for Medicare & Medicaid Services (CMS) ruled that the evidence for VNS was insufficient, blocking Medicare coverage. Typically, when Medicare blocks coverage, so too do the commercial insurance companies. The RECOVER trial’s goal is to settle the coverage question, hopefully making VNS much more readily available.
Led by a team from Washington University in St. Louis, the RECOVER study was initially a one-year, double-blind study of 493 participants across 84 US sites, randomized to active VNS or a sham (unit implanted but not activated). The VNS units, made by the sponsor, LivaNova, were implanted subcutaneously in the chest with a lead wrapped around the left cervical vagus nerve.
The primary endpoint for the research was the percentage of time a participant spent “in response,” defined as a >= 50% improvement on the MADRS, a standard for measuring depression.

The disappointing news from the first-year trial was that there was no significant difference in MADRS scores between the active and sham arms. In contrast, the other measures showed a statistically significant, “modest,” difference between the groups. Conway and colleagues call this out, acknowledging that MADRS may not be the right measure for this population.
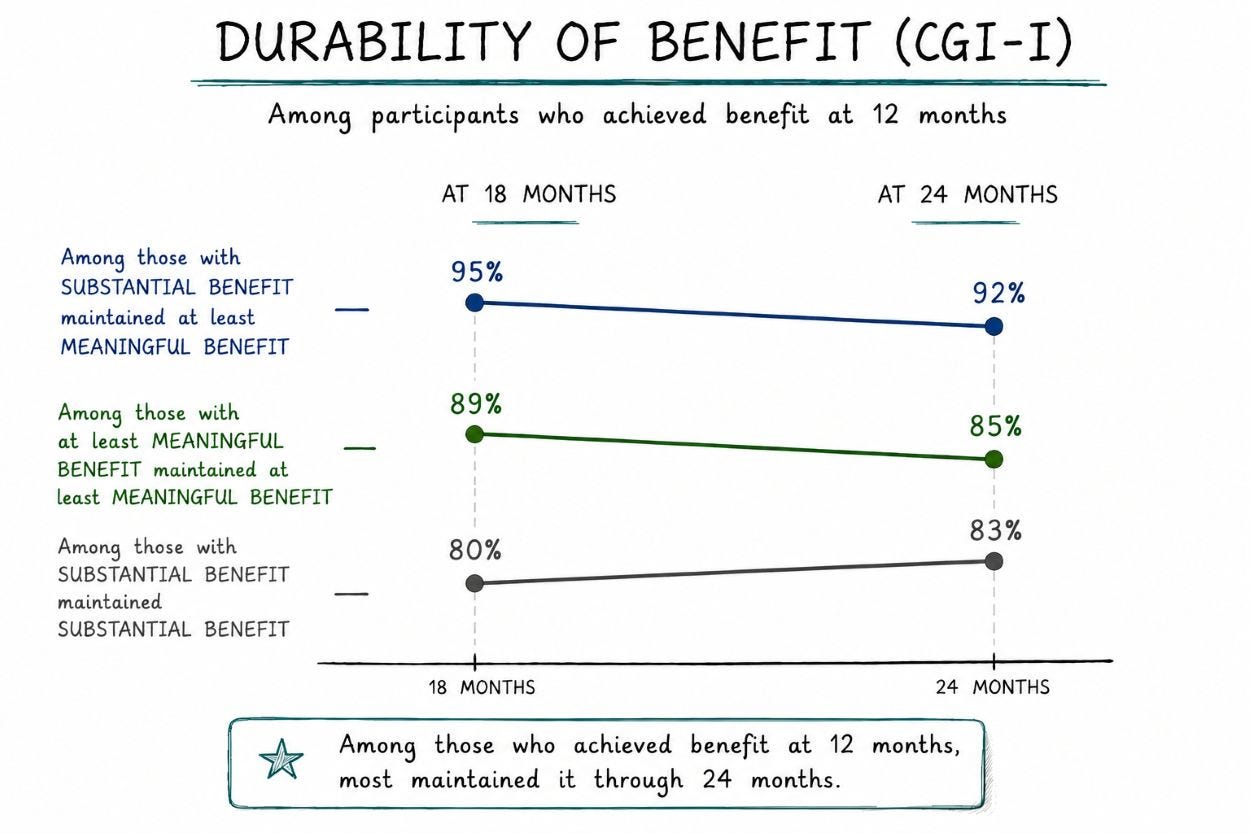
Yet the two-year follow-up study highlights impressive durability. As shown in the chart below, among patients who showed at least meaningful benefit at 12 months, 85% still had it at 24 months. The stronger responders held even better: of those with substantial benefit at 12 months, 92% still had at least meaningful benefit at 24 months. Not shown in the chart, but worth calling out, is that about a third of patients with no benefit at 12 months gained benefit during year two. Relapse was rare, and there were no safety issues.
To interpret these results, it’s important to understand the initial 12-month trial. The trial had two arms. Everyone (493) received an implant and underwent the standard interviews and screenings across four measures: clinician impression (CGI-I), patient self-report (QIDS-SR), a masked, off-site clinician rating (QIDS-C), and MADRS. Half the patients had the device turned on and calibrated over months 1-3.
At the end of the first year, all patients had their devices turned on, but the researchers only included the first-year active group scores in their durability analysis. This decision is a real limitation that we’ll return to below.

“With RECOVER, we might be seeing the flip side of the same biology from Field Note 1, though it’s impossible to verify.”
What grabbed me about the RECOVER results is both the promise of VNS and the challenges of TRD. VNS isn’t a medication targeting neurotransmitters; rather, it’s an intervention that stimulates an entire regulatory system tied to the vagus nerve. This distinction is particularly important for this population, given their lifelong challenges of being continually disappointed by medications.
For me, the obvious question is, given that VNS shows some benefit, what is it doing? Surprisingly, the researchers did not investigate this question. They only speculate on this, with likely candidates including changes in neurotransmitter signaling, neuroplasticity, and the vagus nerve’s anti-inflammatory effects.
The inflammation angle aligns with my first Field Note, where I discussed its role in altering vagal nerve signaling and driving cognitive decline in mice. I understand why RECOVER didn’t measure any inflammatory markers. Its design focused not on how VNS works, but how well it works.
This thread led me to a very small Canadian study by Lespérance et. al. that measured inflammatory markers in TRD patients receiving VNS. This trial comes with two key disclaimers: it involved only 6 patients, and the patients’ level of depression was less severe than that of the RECOVER group.
The Lespérance team found a reduction in inflammatory markers, but not those typically associated with damaging inflammation and depression: TNF-α and IL-6. Neither marker moved noticeably. What changed were other inflammation markers related to signaling pathways that recruit immune cells into the brain, as well as proteins that govern the blood-brain barrier.
The authors interpreted this (pure speculation) to mean that VNS may not directly reduce inflammation; rather, it influences the underlying inflammatory machinery. For example, augmenting the blood-brain barrier and reducing the signals that summon immune cells to cross it.
In Field Note 1, we saw how bacterial metabolites suppressed vagal nerve signaling, leading to neuroinflammation and downstream memory loss in mice. With RECOVER, we might be seeing the flip side of the same biology, though it’s impossible to verify because RECOVER didn’t measure any inflammatory markers, and Lespérance included only 6 patients.
From an upstream perspective, aspects of both depression and cognitive decline might overlap at the intersection of the vagus nerve, the blood-brain barrier, and inflammation. And certainly, there is strong evidence that midlife depression associates with cognitive decline later in life. But does having depression in midlife cause later cognitive decline, or are they both symptoms of the same upstream dysfunction? It’s a question worth revisiting.

“This trial may be telling us more about the limits of how we measure TRD, than how well VNS treats it.”
Plausible isn’t proven, and this section is where I work through the gap with three concerns about how to interpret these results.
First, we don’t know why VNS is triggering the results the authors found. Their best guesses are:
Changes in neurotransmitter signaling would involve the locus coeruleus, a small brainstem nucleus that’s a principal source of norepinephrine and one of the structures that project to the hippocampus, a structure I wrote about in Field Note 1.
Neuroplasticity, which seems to be a catch-all these days for both brain dysfunction and its potential recovery.
The anti-inflammatory pathway.
Second, because there was no control arm in year two, there is no way to tell if durability is due to VNS. Certainly, scores (non-MADRS) remained high and even rose in some cases, but without a sham-control group, we don’t know whether VNS was the reason.
Third, the relationship between the responses of the sham and active stimulation groups is odd. The sham group's scores increased in the last three months of the first-year trial, and the authors speculate that sham participants became more optimistic as the activation date approached. There's clearly much more going on than just vagal stimulation, and even the authors noted that the sham group scored higher than in comparable trials.
On the surface, this research looks like a story about whether VNS works for severe depression, and according to the standard depression scale (MADRS), it doesn’t. My take is that the researchers chose the wrong primary endpoint for patients with TRD. For the meaningful subset of patients who responded on the other three measures, the vast majority maintained that response two years out. Again, these were people who had spent half their lives with treatments failing them. So, while this trial suggests some benefit from VNS, it clearly highlights the challenge of measuring TRD in the first place.

Conway et. al. Vagus nerve stimulation in treatment-resistant depression: A one-year, randomized, sham-controlled trial. Brain Stimulation. 2025;18:676–689.
Conway et. al. Durability of the benefit of vagus nerve stimulation in markedly treatment-resistant major depression: a RECOVER trial report. International Journal of Neuropsychopharmacology. 2026;29:pyaf080.
Lespérance et. al. Vagus Nerve Stimulation Modulates Inflammation in Treatment-Resistant Depression Patients: A Pilot Study. International Journal of Molecular Sciences. 2024;25:2679.

For my next Field Note, I want to further look into the blood-brain barrier and its possible role in cognitive decline and depression. Suffice it to say, it’s time to take out the trash.

If you’re not a subscriber, please subscribe to get full access to the newsletter and publication archives.
Well done article. Thank you.